Clinical TrailsInsmed’s Brensocatib Misses Endpoints in Phase 2b BiRCh Trial for Chronic... Insmed’s Brensocatib Misses Endpoints in Phase 2b BiRCh Trial for Chronic... Read Post »
Lifestyle WellnessAlcohol and Sleeping Pills: Why This Combination Makes Drowsiness Dangerous Alcohol and Sleeping Pills: Why This Combination Makes Drowsiness Dangerous Read Post »
Drugs Safety Alert ResearchFDA Safety Update: Andexxa Risks Outweigh Benefits After Postmarketing Thro... FDA Safety Update: Andexxa Risks Outweigh Benefits After Postmarketing Thro... Read Post »
Clinical TrailsPhase II FALKON Trial Discontinued After Fidrisertib Fails in FOP Phase II FALKON Trial Discontinued After Fidrisertib Fails in FOP Read Post »
New Drug ApprovalMYQORZO Aficamten FDA Approval: Breakthrough for Symptomatic oHCM Treatment... MYQORZO Aficamten FDA Approval: Breakthrough for Symptomatic oHCM Treatment... Read Post »
Clinical TrailsLilly’s Orforglipron Maintains Weight Loss Post-Wegovy/Zepbound in AT... Lilly’s Orforglipron Maintains Weight Loss Post-Wegovy/Zepbound in AT... Read Post »
Clinical TrailsTakeda’s Zasocitinib Hits All Phase 3 Endpoints in Plaque Psoriasis: ... Takeda’s Zasocitinib Hits All Phase 3 Endpoints in Plaque Psoriasis: ... Read Post »
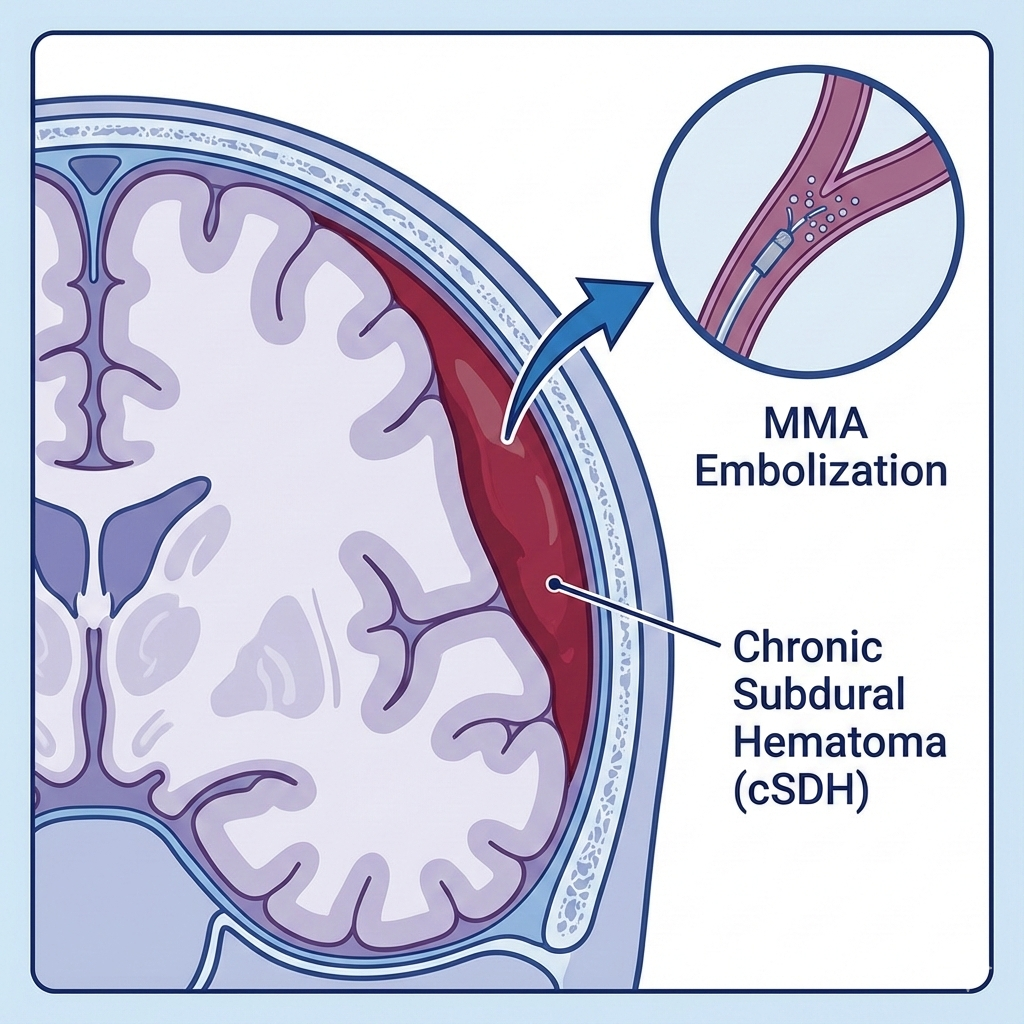
New Drug ApprovalFDA Approves Expanded Indication for Johnson & Johnson’s TRUFILL n‑... FDA Approves Expanded Indication for Johnson & Johnson’s TRUFILL n‑... Read Post »
New Drug ApprovalNovo Nordisk Pushes Obesity Innovation Forward With FDA Filing for CagriSem... Novo Nordisk Pushes Obesity Innovation Forward With FDA Filing for CagriSem... Read Post »
Food WellnessFood, Antibiotics, and the Gut: What Patients Should Know Food, Antibiotics, and the Gut: What Patients Should Know Read Post »
New Drug ApprovalinMIND Trial Success: Minjuvi (Tafasitamab) Now EU-Approved for Relapsed Fo... inMIND Trial Success: Minjuvi (Tafasitamab) Now EU-Approved for Relapsed Fo... Read Post »
Health Tidings ResearchFDA Grants Advanced Manufacturing Technology Designation to Astellas’ Mah... FDA Grants Advanced Manufacturing Technology Designation to Astellas’ Mah... Read Post »
New Drug ApprovalSaphnelo Gains EU Approval for At-Home Subcutaneous Self-Administration in ... Saphnelo Gains EU Approval for At-Home Subcutaneous Self-Administration in ... Read Post »
Health Tidings ResearchBlueRock Therapeutics’ Bemdaneprocel Earns Pioneering Regenerative Medica... BlueRock Therapeutics’ Bemdaneprocel Earns Pioneering Regenerative Medica... Read Post »
Lifestyle Research WellnessCan Smoking Make Asthma Inhalers Less Effective? Can Smoking Make Asthma Inhalers Less Effective? Read Post »
New Drug ApprovalAddyi FDA Approval 2025: Now for Postmenopausal Women with Low Libido Addyi FDA Approval 2025: Now for Postmenopausal Women with Low Libido Read Post »
New Drug ApprovalBreakthrough PCSK9 Inhibitor LEROCHOL Approved for Hypercholesterolemia Breakthrough PCSK9 Inhibitor LEROCHOL Approved for Hypercholesterolemia Read Post »
Clinical TrailsPhase 3 ARTISTRY-2 Data Support Bictegravir–Lenacapavir as a Potential Ne... Phase 3 ARTISTRY-2 Data Support Bictegravir–Lenacapavir as a Potential Ne... Read Post »
New Drug ApprovalExdensur (Depemokimab) Secures First Global Approval in the UK, Followed by... Exdensur (Depemokimab) Secures First Global Approval in the UK, Followed by... Read Post »
Health Tidings ResearchNo Patient Identifiers Needed: FDA Removes a Key Barrier to Using Real-Worl... No Patient Identifiers Needed: FDA Removes a Key Barrier to Using Real-Worl... Read Post »
Clinical TrailsFDA Awards National Priority Voucher to Teclistamab Plus Daratumumab as Pha... FDA Awards National Priority Voucher to Teclistamab Plus Daratumumab as Pha... Read Post »
Clinical TrailsMazdutide Shows Strong Weight Loss and Metabolic Benefits in Phase 1b Trial... Mazdutide Shows Strong Weight Loss and Metabolic Benefits in Phase 1b Trial... Read Post »
Food Research WellnessLove Tea but Taking Iron Pills? Read This First Love Tea but Taking Iron Pills? Read This First Read Post »
Clinical TrailsAmneal’s Interim Phase 4 ELEVATE-PD Data Shows Extended “Good On”... Amneal’s Interim Phase 4 ELEVATE-PD Data Shows Extended “Good On”... Read Post »
New Drug ApprovalFDA Approves CARDAMYST™ (Etripamil) as First Self-Administered Nasal Spra... FDA Approves CARDAMYST™ (Etripamil) as First Self-Administered Nasal Spra... Read Post »
Drugs Safety Alert ResearchWHO Review Shows Strong Evidence That Vaccines Are Not Linked to Autism WHO Review Shows Strong Evidence That Vaccines Are Not Linked to Autism Read Post »
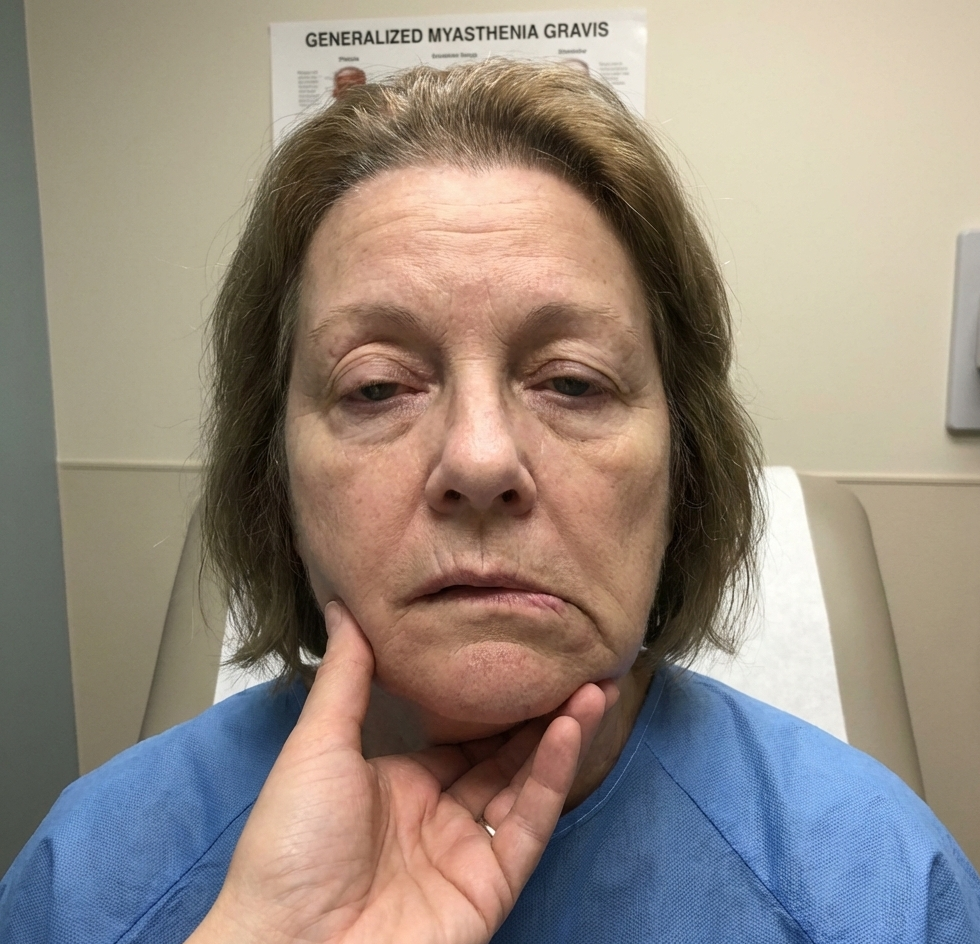
New Drug ApprovalNew FDA Approval: Uplizna for gMG in Adults New FDA Approval: Uplizna for gMG in Adults Read Post »
New Drug ApprovalEMA CHMP December 2025 Meeting: 7 New Medicine Approvals and 12 Indication ... EMA CHMP December 2025 Meeting: 7 New Medicine Approvals and 12 Indication ... Read Post »
Food WellnessDoes Milk Affect Your Thyroid Medicine? Simple Tips for Taking Levothyroxin... Does Milk Affect Your Thyroid Medicine? Simple Tips for Taking Levothyroxin... Read Post »
New Drug ApprovalFDA Approves Nuzolvence (Zoliflodacin): First-in-Class Oral Antibiotic for ... FDA Approves Nuzolvence (Zoliflodacin): First-in-Class Oral Antibiotic for ... Read Post »
Clinical TrailsEli Lilly’s Triple Agonist Retatrutide Hits Phase 3 Goals in Obesity ... Eli Lilly’s Triple Agonist Retatrutide Hits Phase 3 Goals in Obesity ... Read Post »
New Drug ApprovalFDA Approves First Cell-Based Therapy Waskyra for Rare WAS Immunodeficiency FDA Approves First Cell-Based Therapy Waskyra for Rare WAS Immunodeficiency Read Post »
New Drug ApprovalFDA’s First CNPV Approval: Augmentin XR Goes Domestic FDA’s First CNPV Approval: Augmentin XR Goes Domestic Read Post »
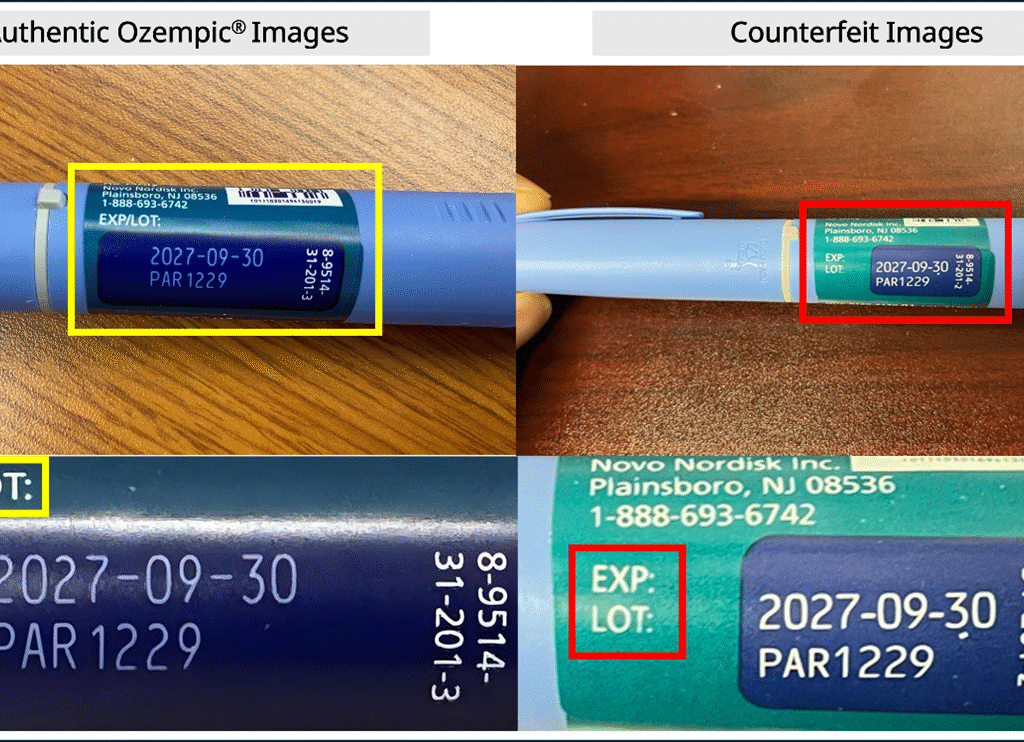
Drugs Safety Alert ResearchFDA Alerts on Fake Ozempic in Legitimate US Supply: Novo Nordisk Guidance A... FDA Alerts on Fake Ozempic in Legitimate US Supply: Novo Nordisk Guidance A... Read Post »
New Drug ApprovalFDA Qualifies First AI Tool under Drug Development Tool Program, Paving the... FDA Qualifies First AI Tool under Drug Development Tool Program, Paving the... Read Post »
New Drug ApprovalFDA Approves Omisirge for Severe Aplastic Anemia: A New Option for Patients... FDA Approves Omisirge for Severe Aplastic Anemia: A New Option for Patients... Read Post »
Clinical TrailsVertex CASGEVY Breakthrough: First Data in Children 5-11 at ASH 2025, Globa... Vertex CASGEVY Breakthrough: First Data in Children 5-11 at ASH 2025, Globa... Read Post »
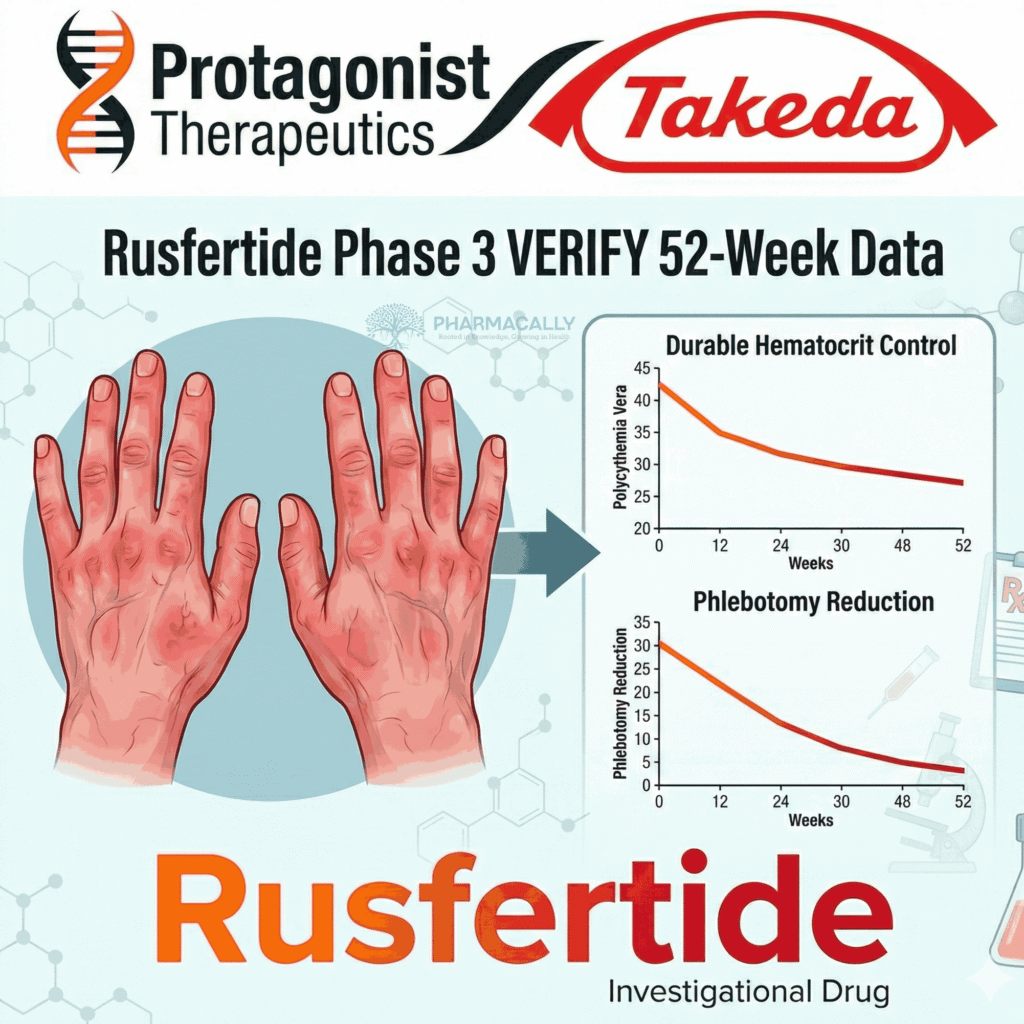
Clinical TrailsBreakthrough Rusfertide Phase 3 VERIFY Results: 52-Week Hematocrit Control ... Breakthrough Rusfertide Phase 3 VERIFY Results: 52-Week Hematocrit Control ... Read Post »
Lifestyle Research WellnessUnderstanding Cannabis: How Medical and Recreational Use Differ in Purpose,... Understanding Cannabis: How Medical and Recreational Use Differ in Purpose,... Read Post »
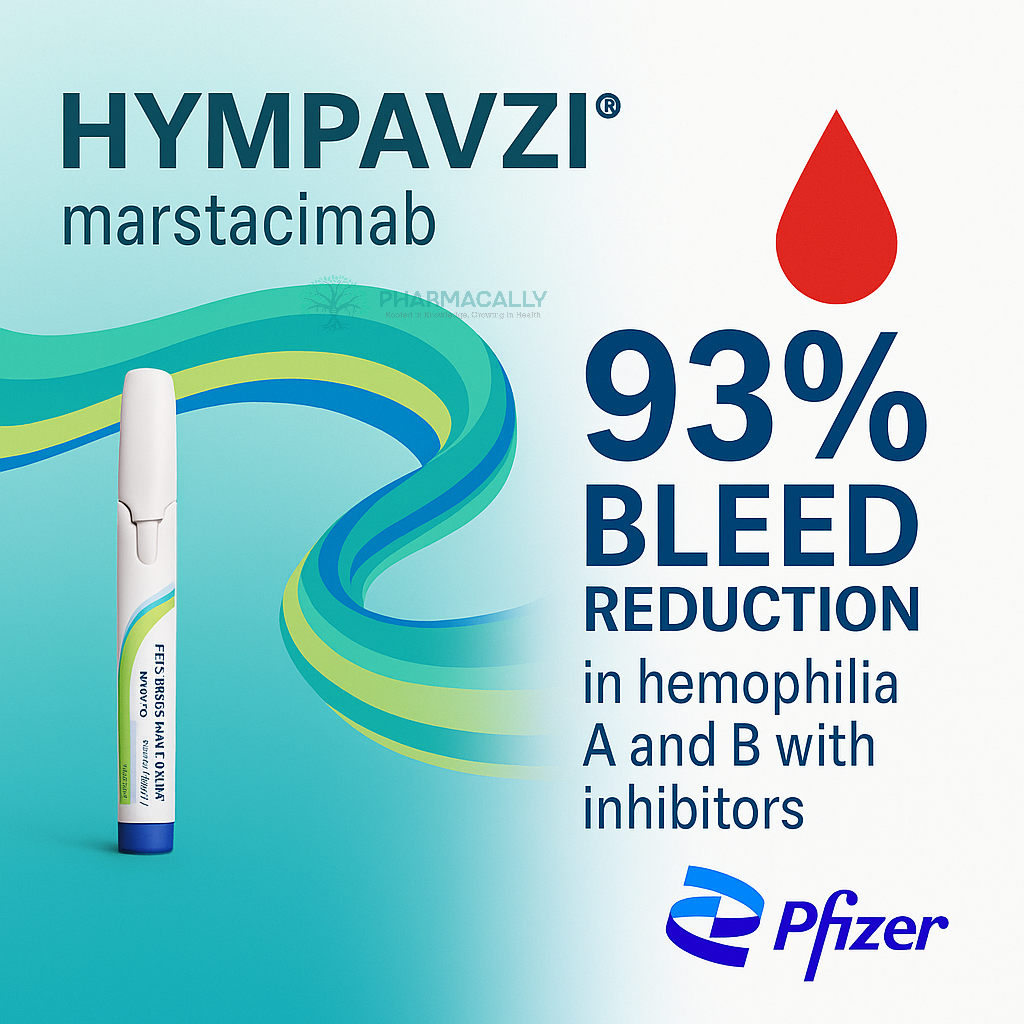
Clinical TrailsPfizer’s HYMPAVZI Shows 93% Bleed Reduction in Hemophilia A/B with Inhibi... Pfizer’s HYMPAVZI Shows 93% Bleed Reduction in Hemophilia A/B with Inhibi... Read Post »
Clinical TrailsZorevunersen Four-Year Results Confirm Disease-Modifying Potential in Pedia... Zorevunersen Four-Year Results Confirm Disease-Modifying Potential in Pedia... Read Post »
Health Tidings ResearchFDA Moves Toward Real-World Evaluation of Digital Devices With TEMPO Progra... FDA Moves Toward Real-World Evaluation of Digital Devices With TEMPO Progra... Read Post »
Clinical TrailsJnJ’s INLEXZO™ Achieves 74% One-Year Disease-Free Survival in BCG-U... JnJ’s INLEXZO™ Achieves 74% One-Year Disease-Free Survival in BCG-U... Read Post »
Clinical TrailsBayer Launches Phase III SUNFLOWER Trial: Mirena 52mg LNG-IUS for Nonatypic... Bayer Launches Phase III SUNFLOWER Trial: Mirena 52mg LNG-IUS for Nonatypic... Read Post »
Clinical TrailsPositive HOPE-3 Phase 3 Results Support Deramiocel as a Potential New Treat... Positive HOPE-3 Phase 3 Results Support Deramiocel as a Potential New Treat... Read Post »
Health Tidings ResearchAbbott Launches Two New Ensure® Max Protein Shakes: 42g Protein and 2-in-1... Abbott Launches Two New Ensure® Max Protein Shakes: 42g Protein and 2-in-1... Read Post »
New Drug ApprovalFDA Approves Breyanzi as First CAR T-Cell Therapy for Relapsed/Refractory M... FDA Approves Breyanzi as First CAR T-Cell Therapy for Relapsed/Refractory M... Read Post »
Clinical Trails New Drug ApprovalIonis’ Zilganersen Earns FDA Breakthrough Therapy Designation for Ultra R... Ionis’ Zilganersen Earns FDA Breakthrough Therapy Designation for Ultra R... Read Post »
Clinical TrailsLEQEMBI® (Lecanemab-irmb) CTAD 2025 Data Confirms Aβ Protofibril Reductio... LEQEMBI® (Lecanemab-irmb) CTAD 2025 Data Confirms Aβ Protofibril Reductio... Read Post »
New Drug ApprovalSun Pharma Launches Ilumya® in India: A Global Innovative Drug for Moderat... Sun Pharma Launches Ilumya® in India: A Global Innovative Drug for Moderat... Read Post »